Seizures
Definitions
- Seizure
- The clinical
manifestations of an abnormal and excessive excitation of a population of
neurons
- Epilepsy
- Recurrent
seizures which are unprovoked by systemic or neurologic insults
- ILAE – “a disorder
of the brain characterized by an enduring predisposition to generate
epileptic seizures”
- Requires the
“occurrence of at least one unprovoked seizure”
Epidemiology:
·
5-10%
of the population will have a seizure in their lifetime
·
25-30%
due to acute brain disturbance
·
30%
of people who ever have a seizure will eventually be diagnosed with epilepsy
Recurrence
rate in acute brain disturbance
- If no structural
damage – less than 3%
- If structural
damage 12.5% (1/8)
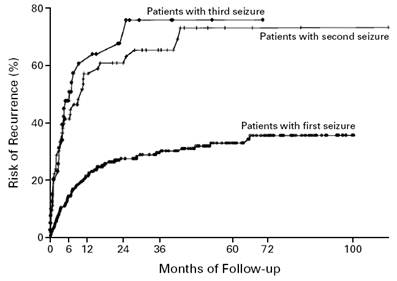
Recurrence
rate if unprovoked:
- After one
seizure 30-50%
- After 2
unprovoked seizures 70-80% -diagnosis of epilepsy
If
a second seizure is to occur 60-70% occur within 6
months
Epilepsy
- Incidence
0.3-0.5%
- Prevalence
0.5-1%
- Lifetime risk
1.4%-3.3%
Seizure
types
and Classification
- Generalized
seizures
- Begin in
bilaterally distributed networks
- Can begin
‘focally’ within a network but do not recurrently originate in the same
region.
- Partial
- Originate in
networks limited to one hemisphere
- The seizure has
a consistent focus of onset.
- Epilepsy
syndromes will be grouped according to aetiology (see Epilepsy Syndromes)
Bold text = new ILAE
terminology
|
Seizures |
Description |
EEG |
|
Partial
(focal) |
Localized
to discrete area’s of the cerebral cortex |
|
|
Simple |
Consciousness
maintained “With observable
motor or autonomic symptoms” Motor
-
Head and eyes turn away from side of focus -
Jacksonian Autonomic “With subjective
sensory or psychic symptoms only” = aura Sensory -
Usually numbness or paraesthsia,
visual relatively rare, auditory and vertiginous can also occur -
Olfactory -
Gustatory -
Visceral Psychic
|
|
|
Complex “With impairment of
consciousness or awareness” |
Decreased
awareness/ consciousness Frequent
aura Automatisms Post-ictal confusion/amnesia Psychic
symptoms can occur -
Illusions, hallucinations, déjà vu, jamis
vu, affective symptoms |
Often
normal Brief
discharges – epileptiform spikes/sharp waves |
|
Partial
with secondary generalization “Evolving to
bilateral convulsive seizure” |
Usually
frontal lobe focus Usually
tonic-clonic seizure |
|
|
Primarily
generalized |
Diffuse
area’s of the brain simultaneously |
|
|
Tonic-clonic |
May
be vague prodrome Most
common seizure in metabolic disturbances Tonic
phase 10-20sec -
Pupils dilated and NR Clonic phase -
8Hz slowing to 4Hz -
~30s -
Ends with deep inspiration Gradually
increasing relaxation Usually
no more than 1min Post-ictal – unresponsive, flaccid, salivation, bowel/bladder
incontinence |
Tonic
phase – progressive increase in generalized low-voltage fast activity
followed by generalized high amplitude, polyspike
discharges. Clonic phase – spike and wave Post-ictal – generalized slowing. |
|
Absence |
Brief,
sudden lapses of consciousness (2-10s) without lapses of postural control No
post-ictal confusion Subtle
movements may accompany Usually
begin in childhood (4-8yrs) 15-20%
of childhood seizures 60-70%
resolve during adolescence 50%
will also experience TC seizure 33%
will have myoclonic jerks |
Generalized,
symmetric 3Hz spike and wave discharge that begins and ends suddenly Hyperventilation
provokes seizures and EEG changes |
|
Typical |
||
|
Atypical |
||
|
With special features |
||
|
Myoclonic |
Most
common with metabolic syndromes, degenerative CNS disease, anoxic brain
injury |
Bilateral
synchronus spike and wave pattern – at time of myclonus |
|
Myoclonic atonic |
|
|
|
Myoclonic tonic |
|
|
|
Tonic |
|
|
|
Clonic |
|
|
|
Atonic |
Brief
loss of tone 1-2 sec with loss of consciousness No
post-ictal confusion |
|
|
Unknown |
|
|
|
Epileptic
spasms |
|
|
Aetiology
:
Causes
in Adults
- Unknown 62%
- Stroke 9%
- Trauma 9%
- Alcohol 6%
- Neurodegenerative
disease 4%
- Encephalopathy
3.5%
- Tumours 3%
- Infection 2%
Causes
of seizure (by age)
|
Noenates (less
than 1 month) |
Hypoxia/ischaemia ICH Acute
infection Metabolic Drug
withdrawal Developmental
disorders Genetic
disorders |
|
Infants
and children (1month
to 12 years) |
Febrile
seizures Genetic
disorders CNS
infection Developmental
disorders Trauma Idiopathic |
|
Adolescents (12-18yrs) |
Trauma Genetic Infection Tumour Drug
use Idiopathic |
|
Young
adults 18-35yrs |
Trauma Alcohol
withdrawal Drug
use Tumour Idiopathic |
|
Older
adults Over
35yrs |
Cerebrovascular
disease Tumour Alcohol
withdrawal Metabolic Alzheimer’s/degenerative
disease Idiopathic |
|
|
|
Aetiology and workup of “First Idiopathic seizures” – see
Specific Epilepsy Syndromes
Patient
Evaluation
History
- Previous
seizures including history of febrile seizures
- CNS lesions
- Trauma, CVA,
tumour, vascular malformations
- Developmental
milestones
- Family history
- Drug or alcohol
abuse
- Precipitating
factors:
- Sleep
deprivation, systemic disease, electrolyte/metabolic disturbance, acute
infection, drugs – legal/illegal, alcohol.
- Note: OSA can worsen
seizure – think of this if well controlled epileptic worsens with age
Symptoms:
- Aura’s or other
associated phenomena not previously diagnosed as seizure
- Behaviour
- Vocal
- Motor
- Eyes
- Motionless
stare – MTLE
- Flickering –
absence
- Deviated –
focal
- Rolled back –
syncope
- Closed –
non-epileptic
- Respiration
pattern
- Autonomic –
drooling, pallor, N+V
- LOC
Post ictal
- Amnesia
- Lethargy
- Confusion
- Sleepiness
- Headache
- Muscle ache
- Tongue biting
- Incontinence
- Transient focal
weakness
- N+V
Physical
examination
- Neurological
examination
- Signs of
infection
- Cutaneous
markers of CNS disease
- Signs of trauma
- Signs of
metabolic disease
- CVS examination
for risk of cerebrovascular disease
Investigations
- Bloods:
- Glucose,
calcium, magnesium, U+E, LFT
- Toxin/drug
screen
- Serum prolactin
- Lumbar puncture
– if meningitis suspected or HIV pos
EEG
- Abnormal in 29%
(range 8 to 50%) of adult patients presenting with first seizure
- Increased
incidence of abnormalities in sleep deprivation
- During event
- Interictal
- 60% are normal
in patients with known epilepsy
Imaging
- CT in emergency
cases, otherwise MRI (although no good evidence)
- A significant
abnormality is present in ~10% of adult patient with first seizure (CT or MRI)
- (Dr Archer) “80%
of significant abnormalities will be detected on CT-B’
Differential
diagnoses
- Migraines
- Psychotic
disorders
- TIA/CVA
- Syncope
- Differentiating
from syncope:
|
|
Seizure |
Syncope |
|
Precipitating
|
Usu
none |
Stress,
valsalva, cardiac event |
|
Premonitory
symptoms |
None
or aura |
Tiredness,
nausea, sweating, tunnelling of vision |
|
Posture |
Variable |
Usually
erect |
|
Transition
to unconciouness |
Usu.
Immediate |
Gradual
|
|
Duration
of unconsciousness |
Minutes |
Seconds |
|
Duration
of tonic or clonic movt. |
30-60
seconds |
Never
more than 15sec |
|
Facial
appearance during event |
Cyanosis,
frothing at mouth |
Pallor |
|
Aching
muscles after event |
Often |
Sometimes |
|
Biting
of tongue |
Sometimes |
Rarely |
|
Incontinence |
Sometimes |
Sometimes |
|
Headache |
Sometimes |
Rarely |
|
|
|
|
Treatment:
- Treatment of
underlying condition
- Avoidance of
precipitating factors
- Anti-epileptic
drug therapy
- Avoidance of
dangerous activities
- Driving
- Operating
machinery or at heights
- Swimming alone
- Treat/screen for
concomitant problems
- Depression
- Overall
effective in 60-70% of patients
Ketogenic Diet
- Effective,
especially in paediatric populations
Surgery
- Temporal lobe
resections
- 60-70% chance
of being seizure free
- Vagal nerve
stimulation
- 50% reduction
in 30-40% of patients
- Deep brain
stimulation
- Under
investigation
First seizure treatment
Focal/Partial
Seizures
- Monotherapy is primary aim
- Carbamazepine is
first line
- Controls 70%
*
|
|
Tonic-Clonic |
Partial |
Absence |
Atypical* |
|
First-line |
Valproic acid Lamotrigine (child bearing
women) |
Carbamazepine Phenytoin Lamotrigine Valproic acid |
Valproic acid Ethosuximide |
Valproic acid |
|
Alternatives |
Phenytoin Carbamazepine Topiramate Zonisamide Felbamate Primidone Phenobarbital |
Topiramate Levetriacetam Tiagabine Zonisamide Gabapentin
Primidone Phenobarbital |
Lamotrigine Clonazepam |
Lamotrigine Topiramate Clonazepam
Felbamate |
|
Avoid |
Ethosuximide Tigabine Vigabatrin |
|
Phenytoin Carbamazepine Tigabine Vigabatrin |
|
*
Atypical absence, myoclonic, atonic
Specific Anticonvulsants
Driving
|
After isolated
seizure |
6 months |
|
Epilepsy – From
initial diagnosis |
6 months |
|
Epilepsy
-Previously uncontrolled seizures |
2
years |
|
Sleep only seizures |
12 months |
|
Post surgery for
epilepsy |
12 months |
|
Seizure due to
identified stimulus in previously well controlled person |
1 month |
|
Stimulus
not identified |
3
months |
|
If
seizure causes MVA |
1
year |
|
Withdrawal of
treatment |
3 months |
|
If
seizure off treatment and treatment restarted |
1month |
Epilepsy
and Suicide
- RR = 2 when all
patients with psychiatric disease excluded
- Highest risk
during first half year after diagnosis
- ? common
pathogenic mechanism in terms of receptor abnormalities
SUDEP (Sudden
unexpected death in epilepsy)
Epidemiology
- Australia ~280
deaths/year
- Mean age of
death from epilepsy 52
- Rates
|
|
Per
1000/year |
|
New
onset epilepsy |
~
0.35 |
|
General
population of epilepsy |
~
0.5-2.0 |
|
Refractory
seizures |
~4.0 |
|
Associated
mental retardation |
~3.0 |
Pathogenesis
·
Respiratory
causes probably important
·
?Cerebral
shutdown
·
Small
proportion cardiac cause (0.1-0.4% of seizures observed to cause asystole)
Risk factors
·
Seizures:
o
GTCS
o
Recent
or frequent seizures (>3 seizures in last year ~8x risk)
·
Medications:
o
Non-compliance
o
Recent
and frequent changes in medication
o
Patients
on polytherapy (polytherapy
and >3seizures ~25x risk)
·
Environment
o
?Lack
of nocturnal supervision/sleeping alone
·
?Alcohol
·
?Depression
- SUDEP NEJM 2011,
SUDEP Lancet 2011
References
“Evaluation
of first seizure” Neurology 2007 69:pg1996-2007
“Initial
Management of Epilepsy” NEJM 2008 359;2 pg166