Stroke
Classification
and Risk factors
Classification – by cause
·
The TOAST classification of aetiology is currently
most used (devised 1991)
|
|
|
Aust* |
|
Ischaemic |
85% |
72.5 |
|
Large artery
(thrombus or embolism) |
50% |
|
|
Small artery |
25% |
|
|
Cardioembolic |
20% |
|
|
Other (rarities) |
5% |
|
|
|
|
|
|
Haemorrhagic |
15% |
14.5 |
|
Hypertensice ICH
|
50% |
|
|
SAH |
25% |
4.3 |
|
Other |
25% |
|
|
Unknown |
|
8.7 |
*NEMESIS study
Full list of causes
Atheroembolism
· Embolism
· Thrombus – occlusive
· Low flow with non-occlusive thrombus
· Dolichoectasia
Small vessel disease
· Standard
· Cerebral amyloid angiopathy
· CADASIL
Rarities
Autoimmune
· Vasculitis
o GCA
o Takayasu’s
o Other – PAN, Wegener’s
o Kawasaki
o Susac’s syndrome
o Cogan syndrome
o Primary cerebral vasculitis
· SLE
· Antiphospholipid syndrome (APLS)
· Behcet’s disease
· HSP
· Essential cryoglobulinaemia
· Sarcoidosis
· Buerger’s disease
Secondary inflammatory vascular disease
· Drugs
· Radiation
· Infections
Non-inflammatroy vasculopathies
· RCVS
· PRES
· Moyamoya
· Fibromuscular dysplasia
· Connective tissue disorders (Marfan, Ehlers Danlos)
Congenital
· Fibromuscular dysplasia
· Hypoplastic carotid and vertebral arteries
· Internal carotid artery loops
Dissection
· Trauma
· Cystic medial necrosis
· Fibromuscular dysplasia
· Syndromes – Marfan, Ehlers-Danlos, Osteogensisis imperfecta
· Inflammation
· Infection (syphilis)
· ADPKD
Haematological
· Hereditary coagulation/thrombophilia
· Sickle cell disease
· PNH
· Essential thrombocytosis
· Polycythaemia
· Paraproteinaemia (hyperviscosity)
· Haematological malignancy
Malignancy
· Malignancy related hyperviscosity
· Direct tumour effects
· Marantic endocarditis
· Chemotherapy treatment
Genetic
· Fabry disease
· AR -CADASIL, CARASAL, RVCL, COL4A1
· AD - Tangier disease, CARASIL, homocystinuria, Sneddon syndrome
· Mitochondrial disease (MELAS)
Misc
· Air, fat or cholesterol embolism
· Migraine
· OCP
· Post angiography
· Toxic effect so venom
· HHT
Risk Factors
Non-Modifiable
·
Age
·
Sex (M>F)
·
Family history
·
Race
Modifiable - definite
·
HTN
·
DM
·
Smoking
·
Alcohol – U shaped, high consumption shows increased
risk
·
OCP
·
Herpes Zoster (especially prior to age 40)
·
Other vascular disease
o
IHD
o
CCF/LVH
o
AF
o
PVD
Modifiable – possible
·
Hyperhomocysteinaemia
- association exists however causality and reversibility unknown
·
Plasma fibrinogen - association exists however
causality and reversibility unknown
·
Haemoglobin level and hyperviscosity
·
Exercise – causality unknown
·
Obesity - causality
unknown
·
Dental procedures – risk increased after recent
procedure
Previous
Cerebrovascular disease
·
A big risk factor for stroke 14% of strokes will have
prior stroke (~1/8)
·
1/8 people with TIA will go on to have CVA within 1
year
|
|
RR |
RRR with
treatment |
NNT PP |
NNT SP |
|
NON-Modifiable |
||||
|
Age (80yrs vs 40yrs) |
30 |
|||
|
Modifiable |
||||
|
HTN |
2-5 |
28-38% |
100-300 |
50-100 |
|
AF |
2-3 (?6) |
68% warfarin 21% aspirin |
20-83 |
13 |
|
DM |
2-6 |
No proven effect |
|
|
|
Smoking |
2 |
50% at 1 year Baseline risk after 5y |
|
|
|
Hyperlipidaemia (esp if <45yo) |
<2 |
10-29% |
|
|
|
Asymptomatic carotid stenosis |
2.0 |
53% |
85 |
|
|
Symptomatic carotid stenosis (70-99%) |
65% at 2yrs |
12 |
||
|
Symptomatic carotid stenosis (50-69%) |
29% at 5yrs |
77 |
||
|
Renal Impairment (eGFR <40) ( BMJ 2010) |
1.43 |
|
||
|
Herpes zoster (esp. age <40) |
~1.7 |
|
|
|
PP primary prevention SP secondary prevention
Clinical
Stroke Syndromes
|
Lacunar |
25% |
|
Anterior circulation |
51% |
|
Partial anterior |
34% |
|
Total |
17% |
|
Posterior circulation |
24% |
Total Anterior
Circulation Infarction (TACI)
· Hemiparesis
o
With/without
hemisensory loss
· Homonymous hemianopia
· Cortical deficit – neglect or aphasia
Partial Anterior
Circulation Infarction (PACI)
· Two out of the three from TACI
· OR isolated cortical deficit
o
Aphasia
o
Predominantly
proprioceptive deficit in one limb
o
Motor/sensory
deficit restricted to one part of body
Lacunar Infarction
- Pure
motor or sensory stroke
Posterior
Circulation Infarction (POCI)
Clinical
Symptoms
· Headache – occurs in ~25% of strokes, more
common in posterior circulation infarcts, may be correlated with site of
injury.
· Seizure – rare (~5%) at time of stroke, more
common with haemorrhage,
o
Presence
of seizure in stroke should prompt consideration of underlying tumour or
encephalitis etc.
·
Gerstmann Syndrome
· Clinical
features
o
Agraphia
o
Acalculia
o
Finger agnosia
o
Left-Right disorientation
· Existence
of the conditions seems controversial
· (Don’t
confuse with another Gerstmann Syndrome related to prions)
· Caused by
lesions in the dominant parietal lobe (usually left)
· In
particular the angular gyrus (junction of the temporal and parietal lobes)
·
Investigations
Investigations - Acute
- CT
- Signs
- Hyperdense MCA – occur in ~50% with
proven MCA occlusion
- Basal ganglia changes
- – loss of definition of the grey matter
best seen at the edge of the caudate capsule
- Cortical changes
- Loss of definition of the insular
ribbon
- CT perfusion imaging
- Standard images show damaged region.
- Perfusion shows area of decreased
blood flow – identifies ischaemic penumbra
- MRI
- Better identification of posterior
fossa, small white matter lesions and vasculitis etc
- Haemorrhage not as clear.
- DWI
- Very sensitive
- ~90% accurate
- False positives – Transient global
amnesia, status, hypoglycaemia, TIA
- False negatives – 2-12%, especially
if very early, more in posterior fossa
- ECG
- AF or evidence of cardiomyopathy
- Bloods – (as per 2010 guidelines)
- FBC
- Electrolytes
- CRP, ESR – inflammatory cause –
infective endocarditis or giant cell arteritis
- LFTs – to diagnose liver disease and
potential coagulopathy, baseline prior to starting statin
- Coagulation profile
- BSL – in case hypoglycaemia is
contributing to the symptoms
- CXR – as a baseline given risk of
aspiration, evidence of cardiomegaly, dissection or malignancy.
Secondary prevention – Investigations
Imaging
·
Carotid
USS
·
MRI
o
Can use
either MRA or Contrast enhanced MRI
o
Cost-effectiveness
studies do not support routine use at current costs
o
Useful
if delayed presentation and doubt about true degree of stenosis if in 50-79%
range.
·
Echocardiogram
o
Cost
effectiveness data do not support its routine use
o
Targeted
use in patients with abnormal ECG or other evidence of thromboembolism etc.
Other
· In addition to acute bloods listed above
· Fasting lipids and BSL
Rare causes/young
stroke bloods
·
Autoimmune
screen
o
ANA
o
ENA
o
APLS
o
Anti-dsDNA
o
ANCA
·
Infection
screen
o
Syphilis
o
HIV
o
HCV
·
Thrombophilia
screen
o
APLS
o
Factor V
leiden
o
Prothrombin
gene mutation
o
Protein
C+ S
o
AT III
deficiency
·
Other
o
SPEP
·
Consider
CSF (vasculitis etc)
·
Genetic/metabolic
testing in selected cases
o
Fabry
testing
Treatment
- acute
Thrombolysis
- Up
to 4.5 hours beneficial
- Up to
3 hours well proven (NINDS, ECAS II)
- 3-4.5
hours shown to be effective (ECASS III trial)
- US
guidelines suggest some exclusions from extended period – age >80,
any warfarin use, baseline stroke score >25, hx of both DM and CVA.
- However
the earlier the better the outcomes.
- Increases
symptomatic haemorrhage 0.6% to 6.4% but does not alter mortality
- Increases
the number of patients with a favorable outcome (mRS 0-1)
- Cochrane
review showed 14% reduction in death or disability (if given within 3
hours)
Aspirin (within 48hours)
- Trials
looked at outcomes at 2-4 weeks and then again at 6 months – IST and CAST
trials (1997).
At 14 days:
- Reduces
death at 14 days (5.0% vs 5.4% - NNT 200, 5/1000)
- Recurrent
ischaemic stroke (2.3% vs 1.6% - NNT 142, 7/1000)
- Further stroke or death (9.1% vs 8.2% -
NNT 111, 9/1000)
- ICH
– 2 extra per 1000 treated
At 6 months:
- 13/1000
more people alive and independent at 6months.
Prevention of aspiration – speech therapy
DVT prophylaxis
- Conflicting
results – some studies show no benefit of heparin, LMWH seems to have
consitently positive effect
- No
increase in haemorrhage with LMWH (high dose heparin/LMWH decreases DVT
more but increases haemorrhage)
- Enoxaparin
better than heparin in one study:
- RR
0.57 (10% vs 18%) PREVAIL study (The
Lancet 2007; 369:1347-1355)
(No difference in haemorrhage b/n groups)
Blood pressure
- No
conclusive evidence of any benefit from blood pressure lowering in the
first 48hours
- Arbitrary
target of less than 220/110 set in guidelines
- Above
this level reduction of 10-20% per day may be attempted with agent of
choice
- Usual
anti-hypertenstives should be given if no contra-indication
Manage cerebral oedema (peaks day 2-3 but can persist ~10days)
- Raise
bed head 20-30 degrees
- Mannitol
– insufficient evidence to recommend
- Glycerol
– evidence of short term benefit with no long term benefit – may be
considered while awaiting surgery
- Hyperventilation
is temporary measure but may also cause vasoconstriction and extend CVA
- Steroids
– have not shown benefit and may cause harm, therefore avoid.
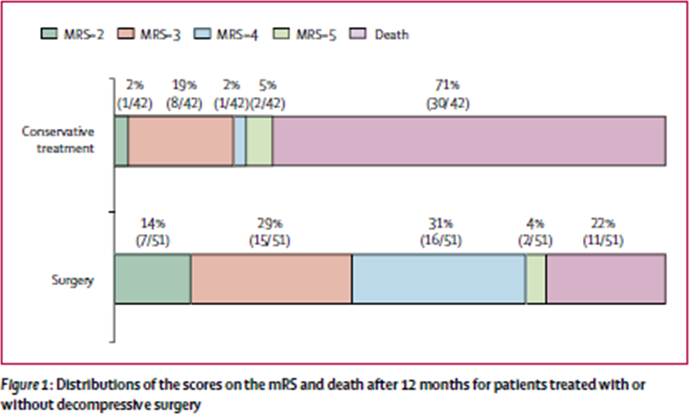
- Decompression
- DECIMAL,
DESTINY, HAMLET trials (and meta-analysis of all three: Lancet Neurol 2007;
6: 215–22)
- Significant
overall increased survival (75% vs 24%, ARR 50%, NNT 2)
- Increases
the number of people who survived with mRS </=3 (NNT 4)
- However
the proportion of survivors with bad score increased – i.e. if
survival, more likely to have poor outcome.
- Note
that average age was ~45yrs in these studies and patients <60years
maximum.
- Decompression
of cerebellar strokes more beneficial.
BSLs – can be disturbed by CVA,
- Should
be monitored in all patients regardless of DM status
- Studies
have shown that high BSL correlated with worse outcome (TOAST study)
- Interventional
studies to prove that tight control improves outcome have negative so far
(but small) GIST-UK
- Recommend
reducing very high BSLs but very tight control unproven
Stroke units
- Large
systematic review (Cochrane 2009)
- Decreased
mortality (ARR 3%)
- NH
care requirement decreased (ARR 2%)
- Death
or dependency OR 0.82
Cooling
- No
evidence that physical cooling helps
- Some
low grade evidence that paracetamol in patients with fever has beneficial
effects on outcome.
Seizures
- Occur
early (<7days) in probably ~3% of patients
- No
evidence for prophylactic anticonvulsant use
- No
particular agent proven superior for recurrent seizures
Secondary Prevention - Interventions
· Risk of
recurrence:
o
43% at 10 years (4%/year)
Anti-platelet agents
Aspirin
o
RRR
~13-20%
Clopidogrel
•
CAPRIE
– clopidogrel vs aspirin in a group of mixed vasculopaths found non-significant
benefit in CVA
Clopidogrel and Aspirin
•
MATCH
– combination of aspirin and clopidogrel post stroke – combination worse (Risk
of life-threatening bleed - 2.6% vs 1.3%)
•
SPS3
(2012) – aspirin and clopidogrel post lacunar stroke – no significant reduction
in stroke, more bleeding.
•
SPS3
subgroup – the addition of clopidogrel to patients who were already taking
aspirin when they had stroke – no benefit
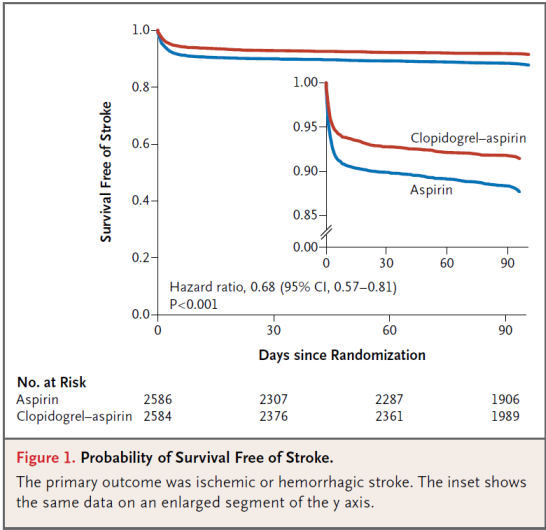
•
CHANCE
trial (NEJM 2013)
o
China,
5170pts with minor stroke (NIHSS </=3 at time of recruitment) or high risk
TIA (ABCD >/=4).
o
RCT
to Aspirin vs Aspirin/Clopidogrel (300mg loading dose +75mg daily starting with
24hours of event)
o
Dual
agent continued for 21 days
o
Stroke
8.2% vs 11.7% (HR 0.68, ARR 3.5% (NNT 29))
o
Haemorrhage
similar in both groups (0.3%)
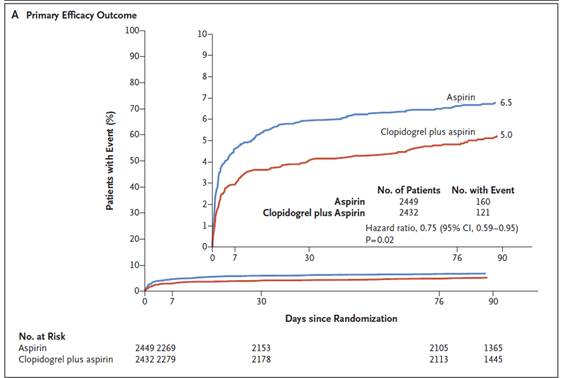
•
POINT
Trial (NEJM 2018)
o
USA/Europe/Aust/NZ
o
Similar
to CHANCE, similar outcomes
o
Aspirin
vs Aspirin/Clopidogrel (600mg loading dose +75mg daily)
o
Primary
outcome - Stroke/MI/vascular death – 5% vs 6.5%
-
ARR1.5%
-
RRR
23%
o
Stroke/MI/vascular
death/major haemorrhage 5.8% vs 6.8%
o
Ischaemic
Stroke – 4.6% vs 6.3%
Aspirin and dipyridamole
•
ESPS-2,
Esprit 06
•
RRR
~ 37%
•
PROFESS
– compared clopidogrel and asasantin
•
no
difference in outcomes
•
greater
proportion of asasantin dropped out due to SE – headache in particular
Warfarin – NOT USEFUL
ULESS AF
•
ESPIRIT
trial (post TIA or ‘small CVA’) – no benefit, more SE.
•
Treat
AF – as per usual guidelines
Hyperlipidaemia
•
Statins
of proven benefit
•
Overall
OR 0.88 (Risk of ischaemic stroke 0.8, Haemorrhagic OR 1.73, thus partially
offsetting benefit)
•
SPARCL
trial – Atorvastatin 80mg
o
Given
to patients who would not otherwise get
statin
o
HR
for stroke 0.84
o
ARR
at 5yrs 2.2%
o
No
mortality difference
o
Increase
in ICH
Blood pressure
•
Recommended
for most – benefit regardless of baseline BP
•
All
agents have shown some benefit except Beta blockers
•
AHA
Guideline 2014
o
Target
<140/90 for all patients
o
Target
<130 systolic for lacunar patients
•
PROGRESS
study
o
Stroke
within 5 yrs (median 8mths), high or high normal BP, given perindopril or
placebo
o
Indapamide
added if necessary
o
Overall
– RRR 28%, ARR 4%
o
Perindopril/indapamide
– bigger decrease in BP - RRR 43%
o
Benefit
regardless of baseline BP
•
PRoFESS
o
Telmisartan
vs placebo with no effect
o
However
BP reduction was only 4/2mmHg
Carotid disease
- Surgery
if appropriate
Smoking
- Increased
risk of stroke essentially disappears 5 years after cessation.
Physical activity
- Proven
in primary prevention but no studies in secondary prevention –
recommended as likely beneficial
Weight reduction
- No
proven benefit
Alcohol
- No
specific recommendations for secondary prevention – see primary
prevention
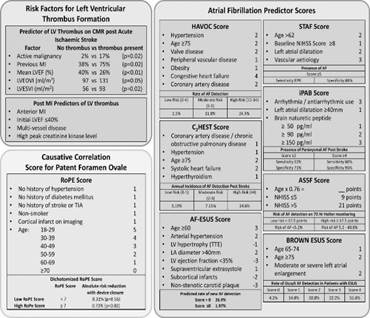
Young
stroke
· >65
(>45 in ATSI)
· Still
largely due to atheroembolic disease however a higher proportion are due to
other causes
· Procoagulant
screen
o
Protein c/s, ATIII, Factor V Leiden, Lupus
anti-coagulant, homocysteine
· TOE –
patent foamen ovale
· MRI – AVM
· CT Angio/
MRA – carotid dissection
Studies
SPARCL
- Atorvastatin after CVA
ESPS-II
EXPRESS study
- Lancet Neurology 2009
- Patients presenting with TIA
- Effect of either direct referral (from
ED) to speciality clinic vs returning pt to GP for subsequent referral to
speciality clinic.
- Decreased admission for stroke at 90
days (2% vs 8%), decreased CVA at 6months, decreased overall hospital
costs.
Thrombolysis
NINDS
- NEJM 2005
- 624 patients within 3 hours
- Reduced deatha and disability by 6.6%
SITS-MOST
- Thrombolysis in practice
- 6500 patients
- ICH 7.3% (3x risk)
- Confirmed benefits – as per NINDS trial
ECASS III trial
- NEJM Sept 25 2008
- Alteplase vs Placebo in 3 to 4.5hour
time period
- Improvement in ‘favourable outcomes’, no
difference in mortality.
SITS-ISTR
- Lancet 2008 372
- Compared outcomes between (3 to
4.5hours) and <3hours – similar safety
References
Series from the Lancet Vol 369 (2007)
CADASIL
·
(Cerebral
autosomal dominant arteriopathy with subcortical infarcts and
leukoencephalopathy)
·
Onset
<50years, median first stroke ~50
·
All
patients with mutation will have MRI lesions by age 35
·
Variable
course – age of onset does not predict rapid course and survival can be long.
Pathology
·
NOTCH3
gene mutations
·
Involved
in smooth muscle cell function
·
Abnormal
protein accumulates within cells in blood vessel walls and has an adverse
effect on their development and response to injury (exact action not clear)
·
Affects
all blood vessels but clinical manifestations limited largely to the brain
·
Rare –
several hundred families worldwide
Clinical manifestations
·
Four
o
Ischaemic
episodes (85%)
o
Cognitive
deficits (60%)
o
Migraine
with aura (30%)
o
Psychiatric
disturbances (25%)
·
Ischaemic
stroke
o
Median onset ~50
o
Classic
lacunar syndromes
o
Unusual
brainstem ‘lacunars’
1.
Pseudobulbar
palsy
·
Cognitive
deficits
o
Essentially
a vascular dementia
·
Migraine
o
Often an
early sign
o
Reduces in
frequency as disease progresses
·
Psychiatric
o
Depression
is major issue
o
Bipolar,
panic and rarely psychosis can occur
o
Apathy
is common
Diagnosis
·
MRI
o
Well
defined typical lacunar infarcts
o
Less
well defined T2 hyperintensities in subcortical white matter – less discrete,
frequently symmetrical
1.
Anterior
temporal lobe lesions in 90%
o
Cerebral
microbleeds also common
o
Brain
atrophy
·
Genetic
testing
·
Biopsy –
skin
o
Characteristic
changes in blood vessel walls (granular osmiophilic material)
Treatment
·
None
·
Treat
other vascular risk factors
·
Triptans
should be avoided in migraine because of increased risk of stroke.
·