Pupils
Physiology
• Iris has two muscles:
o Pupil dilator
- Constriction of this muscle results in pupil dilation (mydriasis)
- Peripherally located
o Sphinctor
- Located more centrally and around edge of pupil
- Constriction causes pupil constriction (meiosis)
• Intrinsically photosensitive retinal ganglion cells (ipRGCs)
o Contain melanopsin
o Only a small number of neurons compared to standard photoreceptors
o Not affected in diseases that affect retinal photorecptors or disease that affect RGC (e.g. LHON
- Thus pupil function remains normal despite severe visual loss
o There is asymmetry of two working hemifields regarding ipRGCs
- Nasal hemifield gives a stronger response than temporal hemifield
- Thus an RAPD can occur with optic tract lesion
• ipRGCs project to pre-tectal nucleus in the midbrain
• Interneurons synapse from PTN bilaterally to Edinger-westphal nucleus (although mainly contralateral
• Parasympathetic fibres travel from EW nucleus to join 3rd nerve
o Run along outer fibres of 3rd nerve.
o 3rd nerve divided into 2 divisions in anterior cavernous sinus – PS fibres follow inferior division into the orbit
o PS fibres synapse in ciliary ganglion
o Cilliary ganglion lies in posterior orbit between lateral rectus and optic nerve
o Post-ganglionic fibres join short ciliary nerves
o Nerves travel to inferior oblique then into the globe between sclera and choroid
o Innervate ciliary muscle and sphincter muscle
o Number of fibres ciliary body:sphincter 30:1
• Near response
o Triad:
- Meiosis
- Accommodation
- Convergence
o Rostral superior colliculus appears to be where this response is coordinated
o Final pathway for Meiosis and accommodation however is still via EW nucleus
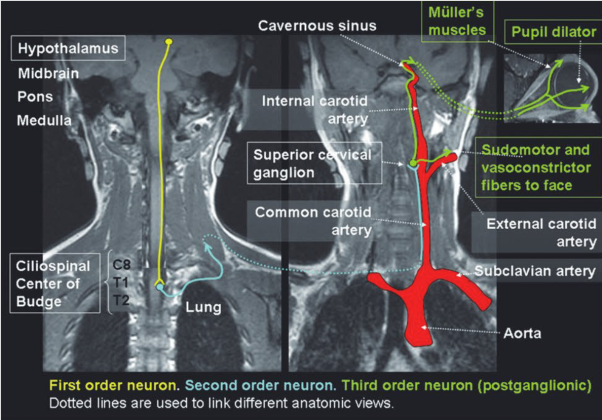
Pupillary dilation
• First order – hypothalamus to spinal cord (C8-T2)
• Second order – exits spinal cord, over the surface of the lung, up along the carotid artery
o Synapses in superior cervical ganglion
• Third order
o Follows carotid up to and through cavernous sinus
o Follows 6th nerve
o Then 5th (nasocilliary branch)
o Then long ciliary branch into the orbit
o Synapses on dilator muscle
o Adrenergic – causing contraction of muscle and pupil dilation.
Examination
• Size
• Equal/anisocoria
o Light
o Dark
• Dilation in dark
• Reactive to light
• RAPD
• Constriction at near
• Examine condition of iris –
o Irregular edge suggesting trauma
o
Testing
Cocaine
• Blocks NA reuptake
• Requires intact sympathetic fibres
• Will have no effect if sympathetic fibres not present or functioning
Apraclonidine
• Direct alpha receptor agonist
• No effect on eyes with intact sympathetic innervation
• Mild pupillary dilation in eyes with sympathetic denervation – regardless of lesion location
• Reverses the Horner syndrome – confirms diagnosis
Hydroxyamphetamine
• Releases stored NA form the postganglionic adrenergic nerve endings
• Causes pupillary dilation in eyes with intact sympathetic innervation
• Has no effect on third order Horner’s
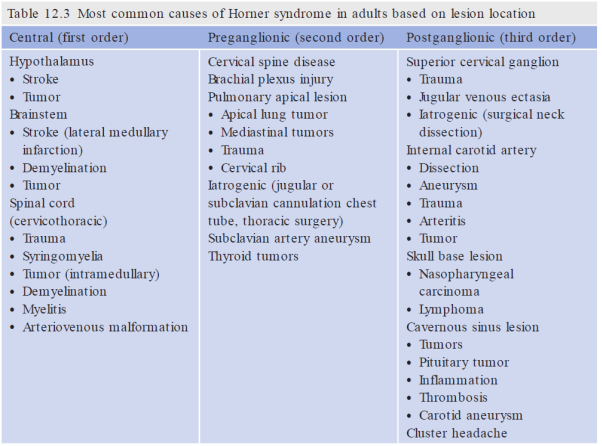
Imaging
First order
- CXR
- CT Chest
- MRI head and neck
- MRA/CTA
Third order
MRI brain
• )
Bilateral poorly reactive pupils
• Dorsal midbrain lesion
o With upgaze palsy
• Miller fisher
• Botulism
• DM
•
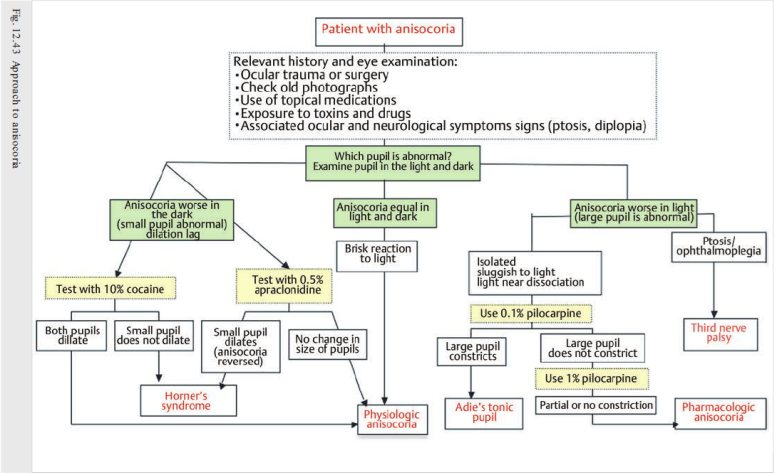
Small pupil abnormal (failure to dilate)
Causes:
• Iris abnormality
• Horner’s
• Physiological
• Pharmacological
Large pupil abnormal (failure to constrict)
Causes
• Third nerve palsy
• Tonic pupil
• Pharmacological
o Iatrogenic – e.g ipratropium
o Plants
• Damaged iris sphincter
o Glaucoma
o Iritis
Third nerve palsy
See
N.B. It is very rare to see an isolated anisocoria in a 3rd nerve palsy (in an alert patient)
Tonic Pupil
Pathophysiology
• Damage to the ciliary ganglion or short ciliary nerves
• Partial preservation of the parasympathetic fibres results in sectoral paralysis
• Light -near dissociation - ?due to larger percentage of fibres to accommodation
Causes:
• Adie (or Holmes Adie) syndrome
o Tonic pupils
o Loss of deep tendon reflexes
o If combined with segmental anhidrosis = Ross syndrome
• Local ocular processes affecting ciliary ganglion
o Orbital trauma, sarcoid, viral, GCA, strabismus surgery, orbital tumours, laser photocoagulation
• Autonomic dysfunction
o Long list of associated autonomic conditions – including syphilis, severe DM, amyloid…
• Idiopathic
Presentation
• Asymptomatic anisocoria
• Painless
• May be difficulty reading
• Difficulty refocusing from near to far
• Photophobia
Examination
• Anisocoria – worse in the light
o N.B. after 1-2 months a tonic pupil may become miotic and smaller than fellow pupil
• Light-near dissociation
o Occurs 8 weeks after denervation, due to abberant reinnervation by accommodative fibres onto iris
• Tonic redilation
• Sectorial paralysis
• Vermiform movements of the iris
• Loss of pupillary ruff
• Depressed corneal sensation
• Bilateral in 10%
Testing
Dilute pilocarpine test
Pilocarpine is a mACh R agonist
Testing
RPR, ANA, ACE, ESR, BSL