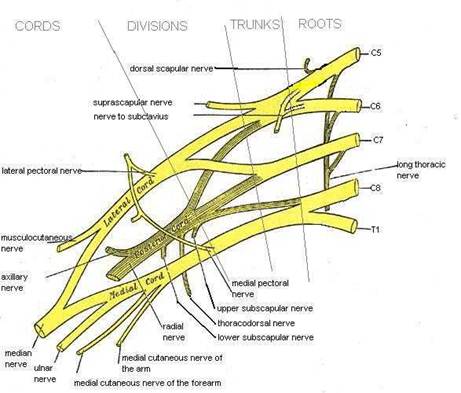
Brachial Plexus and
Shoulder Neuropathies
Upper Trunk
- Erb’s or
Erb-Duchenne palsy
- Loss of C5
and C6
- Most common
brachial palsy
Clinical
- Weakness of:
- shoulder
abductors
- external
rotators
- Elbow
flexors
- Supinator
- Variable
partial weakness of:
- Wrist extensor
- Elbow
extensors
- Some muscles
around the scapula
- Sensory
deficit
- Shoulder
- Lateral
aspect of arm
- May be no
sensory deficit
Treatment
- Better
prognosis than lower injuries, >50% recover completely
Lower Brachial
Plexus
- Klumpke’s or
Dejerine-Klumpke palsy
- Loss of
conduction from T1 and sometimes C8
- Rarer than
upper (Erb’s) palsy
Clinical
- All of the
small muscles of the hand are affected
- The long
finger flexors are sometimes affected
- Wrist flexors
rarely affected
- Triceps
usually spared
- Horner’s syndrome
can occur
- Sensory
deficit – ulnar portion of the hand and forearm
Causes
- Trauma
- Compression
injuries
- Back-pack
palsy – usually upper plexus
- Thoracic
outlet syndrome – usually lower
- Cervical
rib and scalene syndrome
- Hyperabduction
syndrome
- Costoclavicular
syndrome
- Compression
during surgical procedure (especially with shoulder braces)
- Malignancy
- Pancoast
tumour of the apex of the lung
- Usually
presents with horners syndrome and lower brachial plexus injury
- Radiation
injury
- Can be due
to direct injury or scarring of adjacent structures
- Upper or
lower affected
- Can occur up
to 1-2 years after radiation
- Pain is
often a prominent symptom
- Differentiating
from tumour regrowth
|
|
Cancer |
Radiation |
|
Severe pain |
80% |
20% |
|
Part of plexus |
Lower (75%) |
Upper (75%) |
|
Horners syndrome |
Common |
Uncommon |
|
Lymphoedema |
Uncommon |
Common |
|
Time since radiation |
<1year |
>1year
(unless >60Gy) |
- Brachial plexus neuritis
- Also called
neuralgic Shoulder Amyotrophy or Parsonage-Turner syndrome
- Inflammatory
condition of the plexus
- ?Cause –
autoimmune mechanism postulated
- Often a
triggering event such as infection, surgery or vaccination
- Young
adults, M>F
Clinical
- Acute onset
- Severe
shoulder pain is common
- Weakness
within hours or days
- Usually upper
plexus (and/or middle)
- Shoulder
girdle and upper arm
- Winging of
scapula
- Distal
weakness is rare
- Pain usually
abates within a few days leaving the weakness
- Sensory
changes present in variable number (? only 25%)
Diagnosis
o
NCS and EMG can be used to air diagnosis
Treatment
- Good
prognosis
- Severe pain
resolves with a week in 50% and 3months in the rest
- Weakness
resolves slowly starting at 9-12months and taking up to 2 years.
- Glucocorticoids
are sometimes trialled but no evidence to support routine use.
Long Thoracic Nerve
- Pure motor
nerve to serratus anterior(C5-C7)
- Serratus runs
from ribs laterally to anterior surface of scapula
- Weakness
causes winging of scapula
- Multiple
potential causes of injury, often traumatic
Axillary nerve
- C5-C6, innervates
deltoid and teres minor muscles (ext rotation of humerus)
- Sensory
innervation to lateral shoulder
- Affects
flexion, abduction and external rotation of the shoulder.
- Commonly
injured by anterior dislocation of the shoulder
Suprascapular nerve
- C4-C6, innervates supraspinatus and infaspinatus
- Weakness of shoulder abduction and external rotation
- No sensory deficit
- Carries nerve fibres from glenohumeral and AC joints
- Often painful
- Compression of nerve in scapular groove (or coracoids scapular notch) is common.
- Results from repetitive stretching – weight lifting, volleyball
- Usually improvement within 6 weeks of modification of activity
- Steroid injection can be done if severe pain.