Eye Examination - Eye Examination
Anatomy diagrams




Examination – screening
CNI
·
Best to just ask if patient has problem with smell
CNII
·
Acuity
- Fields +/- blind spot
- Fundoscopy
CNIII, IV, VI
·
Eye movements
- Accommodation
- Saccades
CNV
·
Sensation in three divisions
- Pain and light touch
- Corneal reflex
- Efferent CN V
- Afferent CN VII
- Motor
- Masseter contraction
o
Jaw opening
- +/- Jaw jerk
CNVII
·
Facial strength
- Taste anterior two thirds of tongue
CNVIII
·
Hearing
CN IX, X
·
Palate symmetry
- Uvala asymmetry
- Voice
CN XI
·
Head rotation
- Shoulder Shrug
CN XII
·
Tongue protrusion
Multiple Cranial Neuropathies
• Malignant
o Carcinomatous or lymphomatous meningitis
o Metastases
o Local tumour invasion – nasopharyngeal tumour, sarcoma, cordoma
o Perineural invasion – SCC, BCC
• Infections
o Radiculitis/meningeal infections - TB, fungal, syphilis, lyme
o Direct neural infection – Listeria, HIV, CMV, Herpes zoster
o Botulism
• Inflammatory
o Sarcoid
o Wegener granulomatosis
o Sjogren syndrome
o Mixed connective tissue disease
• (Myasthenia gravis)
• Idiopathic
o Tolosa-Hunt like syndrome
o Melkersson-Rosenthal syndrome
o Idiopathic pachymeningitis
o Post-infectious – GBS type
• Vascular
o Carotid dissection or Jugular occlusion at the skull base
• Other
o Trauma
o Paget disease of skull base
o Arnold Chiari malformation
CN I – Olfactory
Course
• Cribriform plate to medial temporal lobe on same side
Examination
• Loss
of smell
• Test each nostril with familiar smells
Lesions
• Causes of anosmia – most are bilateral
• URTI
• Smoking
• Age
• Ethmoid tumours
• Basal skull fractures or frontal fracture
• Post-pituitary surgery
• Congenital
• Frontal lobe base disease
• Meningioma of the olfactory groove
• Post basal meningitis
• Sarcoidosis
Eye Examination - Eye Examination
CN II – Optic
Course
• Retina – optic nerve – optic chiasm
• Optic tract – lateral geniculate body
• Optic radiation – visual cortex
• Light reflex fibres – branch off optic tract to superior colliculus (and synapse with fibres of third nerve)
Examination
• Acuity
• Fields
o Hat pin
o Glasses off
o Fields then map scotoma
• Fundoscopy

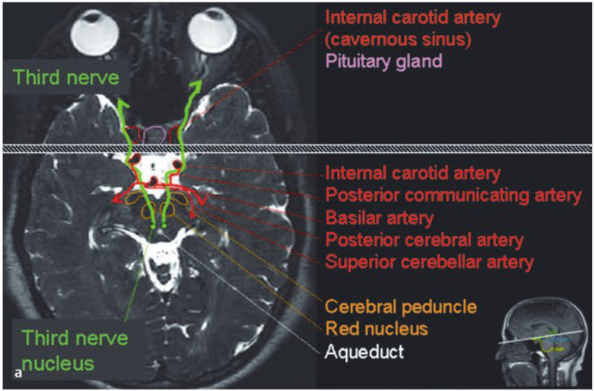
CN III – Oculomotor
Anatomy
• Nuclei - peri-aqueductal grey matter in mid-brain at level of superior colliculus
o Most subnuclei supply ipsilateral functions
o The superior rectus fibres travel contralaterally (roughly through the opposite SR nucleus)
o Both leveator palpebrae are served by a single midline nucleus
• Visceral (Edinger-Westphal nucleus)
o Lies dorsal to somatic nucleus
o Supplies cilliary dilation and cilliary muscles (accommodation)
• Nerve exits anterior midbrain near cerebral peduncle
• Travels between superior cerebrallar artery and PCA
• Travel along PCOM and lateral to ICA
• Into cavernous sinus – lateral wall
• Enters orbit via superior orbital fissure and annulus of Zinn.
• Divides into:
o Superior division – levator palpebrae and superior rectus
o Inferior division – medial rectus, inferior rectus, inferior oblique, ciliary ganglion (parasympathetics)
Function
• Pupils
o
Third nerve supplies parasympathetic fibres to
the pupil via Edinger-Wetphal nucleus – cilliary dilation and papillary accommodation.
o
Sympathetic supply comes via ascending
sympathetic fibres from the spinal cord (C8-T2)
• Eye
movements
o
Supplies all muscles except lateral rectus and
superior oblique
• Other
o
Levator palpebrae –
elevates eyelid


Examination
• Ipsilateral weakness of:
o Adduction
o Elevation
o Depression
• Also:
o Ptosis
o Pupillary dilation
o Accommodation paralysis
• Eye will sit down and out due to unopposed action of lateral rectus and superior oblique
Assess:
• Is it isolated?
o Associated signs will loacalise – e.g. rare for a brainstem/nuclear cause to be isolated
• Is it painful?
o The nerve has sensory fibres (from CNV) which travel with it in the subarachnoid portion
o Microvascular or compressive cause
• Is it complete or partial?
• Is it pupil sparing? (only comment if also a complete CNIII palsy)
o Pupil involvement may suggest a compressive cause
o If there is a complete palsy with pupil sparing then it is highly likely to be microvascular (but can only be assumed if CNII is complete otherwise)
Lesions
Nuclear lesions
• A complete unilateral lesion would cause:
o Ipsilateral complete 3rd nerve palsy
o Bilateral ptosis
o Bilateral elevation deficit
o Often bilateral pupil dilation
• Isolated lesions of the levator or edinger-westphal nucleus can very rarely occur and tend to cause bilateral symptoms
Causes:
• Ischaemia (perforating branches of basilar artery)
• Haemorrhage, tumour, inflammation
Fascicle lesions
• Usually present with other signs given nerve passes close other structures:
o Red nucleus – contralateral tremor (Benedikt’s syndrome)
o Cerebral peduncle – contralateral hemiparesis (Weber’s syndrome)
o Cerebellar peduncle – ipsilateral ataxia (Nothnagel’s syndrome)
o Tremor and ataxia (Claude syndrome)
• Causes:
o Infarction, haemorrhage, neoplasm, demyelination
Nerve lesions in subarachnoid space
• Pupil only (very rare)
o Aneurysm
o External compression from other mass or herniation of uncus
o Intrinsic nerve lesions (schwannoma)
o Infection (basal meningitis)
• Third nerve including pupil
o Aneurysm
o Trauma
o Ischaemia (20%)
o Carotid cavernous fistula
o Mass
o Intrinsic lesion
o Infection
• Third nerve sparing pupil
o Ischaemia
o Compression
o Inflammation
o Infiltration
Nerve lesions in cavernous sinus and superior orbital fissure
• Variable involvement of
o Third
o Fourth
o Sixth
o V1 and V2
o Sympathetic paralysis
Nerve lesions in orbit
• Can selectively affect the superior or inferior division
• Are usually associated with other symptoms – e.g. optic nerve compression or proptosis
CN
IV – Trochlear
Anatomy
• Nucleus, caudal to CNIII nucleus – periaqueductal grey matter at level of inferior colliculus in midbrain.
• The only cranial nerve to emerge dorsally from the brainstem
• Crossed over after emerging
• Travels ventrally and thus has longest course of all cranial nerves (75mm)
• Passes b/n superior cerebellar artery and PCA
• Travels through cavernous sinus
• Supplies superior oblique – intorts the eye, also depression and abducts
Clinical
•
Diplopia
is common, especially when looking down (going down stairs and reading)
o
Vertical
or oblique diplopia
•
Head
tilt to contralateral side to compensate and maintain binocular vision
Examination
•
May
be head tilt away from side of lesion
•
Elevation
(hypertropia) of the affected eye
•
Worse
when looking away from the affected side
•
Unable
to move eye in and down
•
Examination
findings are greater with head tilted to side of lesion.
•
In
patients with CNII lesion it may be hard to tell if IV is intact
o
Ask
patient to abduct eye affected with CNII palsy and then watch for subtle
intorsion as they try to look down
Lesions
•
Most
common causes
o
Trauma
-
Posterior
decussation (close relationship with tentorium)
o
Decompensation
of congenital CN IV lesion
o
Microvascular
ischaemia
•
Other
causes by location
|
Location
of lesion |
Associated Sx |
Causes |
|
Nucleus (midbrain) |
Contralateral
Sup Oblique weakness and Ipsilateral Horners |
Trauma Infarction Neoplasm |
|
Fascicle |
Rare Contralateral
ataxia |
Superior
cerebellar peduncle pathology |
|
Subarachnoid space |
Isolated |
Trauma Microvascular Meningitis Tumour Aneurysm
(rare) |
|
Cavernous sinus |
See
Cavernous sinus syndrome |
|
|
Orbital apex |
See
orbital apex syndromes |
|
|
|
|
|
Decompensated congenital CNIV
• Complaints of torsion less common than acquired
• Overaction of ipsilateral inferior oblique muscle (as compensation from chronic lesion)
• Large vertical fusional amplitude
• Symptoms often arise from breakdown in vertical fusional capability (rather than worsening 4th nerve function)
Bilateral CNIV palsy
• Alternating hypertropia, high degree of excyclotorsion, V-pattern esotropia
• Usually due to trauma or lesion/tumour at site of emergence from posterior brainstem
Treatment of CNIV palsy
• Prism lens (base down)
• Temporary occlusion of lower half of lens on affected side
• Surgery
CN VI – Abducens
Anatomy
• Nucleus – in the centre of the pons, beneath the floor of the 4th ventricle, adjacent to CNVII
• Exits brainstem anteriorly at ponto-medullary junction
• Runs up the front of the brainstem
• Past basilar artery, over crest of petrous part of temporal bone (point of compression in raised ICP)
• Through cavernous sinus, superior orbital fissure
• Supplies lateral rectus
Examination
• Inward deviation of eye (esotropia)
• Can sometimes appear comitant
• One and a half syndrome
o CN VI and ipsilateral MLF lesion
o Either eye unable to look to side of lesion, only contralateral eye able to look away from lesion.
Lesions
• Common and specific causes
o Raised ICP
o Low ICP – especially with spinal CSF leak which may cause downward pressure.
o Microvascular
o Congenital (Duane or Mobius Syndrome)
• Bilateral disease
o Raised ICP
o Meningitis
• Mimics
o Thalamic esotropia
o Convergence spasm
Causes by location
|
Site |
Associated Sx |
Causes |
|
Nucleus (pons) |
Conjugate gaze
palsy (One and a half syndrome) Ipsilateral CNVII |
Stroke Neoplasm |
|
Fascicle (pons) |
Contralateral
hemiparesis +/- other signs |
Stroke Neoplasm Demyelination |
|
Subarachnoid
space |
Isolated |
Microvascular Raised ICP (or
low ICP) Meningitis Trauma Tumour Petrous apex
infection Vertebral/Basilar
dilation/aneurysm Chiari
malformation |
|
Cavernous sinus |
See cavernous
sinus syndrome |
|
|
Orbital Apex |
See Orbital apex
syndromes |
|
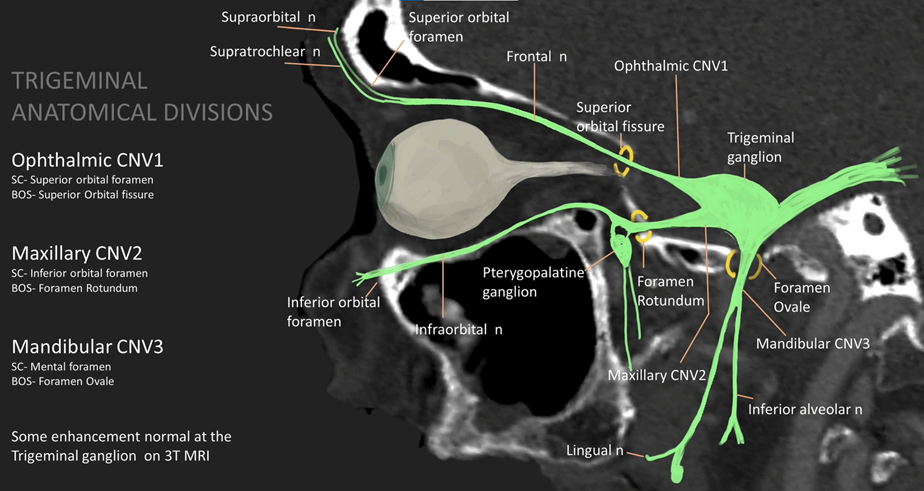
CN V – Trigeminal
Examination
• Sensation
• Corneal reflex
• Masseter contraction
• Jaw opening – deviates to side of lesion
CNVII
(See facial nerve/Bells palsy topic - Bells Palsy)
Functions
• Muscles
• Taste on the anterior two-thirds of the tongue
• Lacrimal and salivary glands
Examination
• Muscle function
• Taste on tongue
• Lacrimation (schirmers test)
CN VIII – Vestibulocochlear
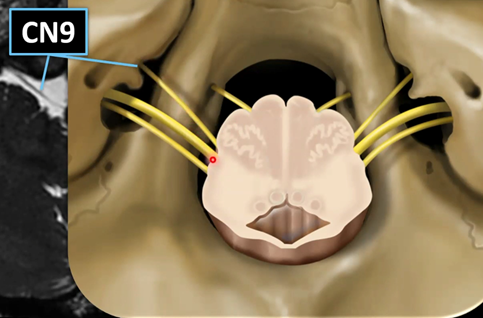
CN IX – Glossopharyngeal
Nuclei
• Medulla
Course
• Formed by rootlets from groove between olive and inferior cerebellar peduncle
• Travels closely with vagus and exits at jugular foramen
Function
• Sensory
to pharynx and larynx with vagus
• Minor motor to pharynx and larynx
• Taste from the posterior third of the tongue
• Stylopharyngeus is the only skeletal muscle innervated
• Carotid baroreceptors (Hering nerve)
Clinical
• Dysphagia, choking
• Often with hoarseness due to vagus nerve damage
Examination
• Elevation
of pharynx (vagus and glossopharyngeal)
• Decreased
saliva production (never actually tested)
• Test
for bilateral sensation to the pharynx and posterior tongue, this may also
elicit a gag reflex
• Asymmetry
of gag reflex is most indicative of pathology (sensory component of reflex is
glossopharyngeal, motor is vagus)
Lesions
• Medulla infarction
• Tumour near jugular foramen – will affect vagus as well
• Internal carotid aneurysm or jugular bulb thrombosis
• Vincristine toxicity – jaw pain


CN X – Vagus
Vagus – name = wanderer
Nuclei
• Motor – nucleus ambiguus of the medulla
• Parasympathetic – dorsal motor nucleus of the vagus in the brainstem
Course
• Rootlets attach to lateral aspect of medulla, caudal to glossopharyngeal
• The branchial motor fibers leave the vagus nerve as three major branches:
o
Pharyngeal branch![]()
o
Superior laryngeal nerve![]()
o Recurrent laryngeal nerve
Function
• Sensation
o Pharynx
o Larynx
o Oesophagus
o Taste (to some extent from soft palate and pharynx, most taste is tongue)
o Tymanic membrane, external auditory meatus
o Chemoreceptors in aortic bodies
o Baroreceptors in aortic arch
• Motor
o Soft palate
o Palatoglossus muscle of the tongue (rest of tongue is hypoglossal)
o Pharynx
o
Larynx – except stylopharyngeus
muscle (CN IX) and the tensor veli palatini muscle
(CN V).
o Upper oesophagus
• Parasympathetic
o Wide distribution – CVS, GIT, Respiratory
Clinical
Examination
• Elevation of palate
• Deviation of uvula
• Gag reflex (efferent arm)
• Voice – hoarse
• Cough – bovine

CN XI – Accessory
Function (pure motor)
• SCM
• Trapezius
CN XII – Hypoglossal
Function
• Motor – Tongue muscles
o
Except for palatoglossus (Vagus)
Examination
• Inspect tongue for wasting and fasciculations (lower motor neurone lesion)
• Protrude tongue – deviates towards weaker side